Twenty three and a half hours
I love this video. Most of my readers do more than 30 minutes, but let’s say you can’t get to the gym, or you’re injured. Or you’re just not in your workout groove. There’s making gains, which is what we’re always trying to achieve, but sometimes, you have to take victory during times of stress to just not go backwards. So if you do nothing else, know that 30 minutes a day is positively associated with many benefits. Read More...
Toe-ing the line: What I think about this whole shoe thing
 Oldest discovered leather shoe: 5500 years old
Oldest discovered leather shoe: 5500 years old
I’ve had a few emails asking me to review some of the literature on the new shoe trend. Every company is jumping on the bandwagon to create their version of the Vibram five TOE shoes (sorry, I’m going to be a hand and wrist sub-specialist. Toes are NOT fingers). It’s a little reminiscent of the “body-toning” shoe thing, without all of the wildly outrageous claims, and a trend that I think will live long enough to warrant weighing in on. Most studies to date have really focused on how the shoes alter foot and gait biomechanics. I would argue that most of the claims on the Vibram website are still largely unsubstantiated or just what I call “motherhood statements”, like: “Eating your greens is good for you,” and “Puting on your jacket when it’s cold outside is good for you.” (basically, statements that don’t really have any clout one way or another, but just make you feel better.) Read More...
What will your legacy be?

There are a lots of things we take for granted. In medicine, this is highlighted every day. It’s not just walking or the ability to do things, but also even basic life functions like eating, talking, and breathing; and some cases, just appearing “normal”. There are days when I’m just happy my patient has a regular heart beat–I’m not even shooting for independent breathing or even independent blood pressure.
The reality is that if you’re reading this, and any part of this blog, you’re fairly healthy, mobile, and possessed of your mental faculties enough to read. You have the ability to enact change in your life. If you’re sitting on the fence, you’re choosing to sit there. Read More...
Why isn’t overeating an eating disorder?
My position on the proposed “Muscle Dysmorphia” remains unchanged. I do not feel it belongs in the DSM in its current state, largely due to the subjective criteria for its proposed diagnostic criteria, which depends entirely on whether the diagnostician feels the patient is already “muscular enough”. Read More...
Fitness, nutrition and a Peruvian fruit stall
 I’m in Peru right now on a volunteer hand surgery assignment. I arrived here about a week ago and when I went to the grocery store the day after I landed to stock up on some supplies, I noticed things in the store that were familiar and things that weren’t so familiar.
I’m in Peru right now on a volunteer hand surgery assignment. I arrived here about a week ago and when I went to the grocery store the day after I landed to stock up on some supplies, I noticed things in the store that were familiar and things that weren’t so familiar.
In an effort to ensure I wasn’t going to get scurvy, I felt like I had to buy some fruit. There were oranges and pineapples and mangos and papayas, but I also wanted something portable that I wouldn’t have to peel or cut or scoop. So I opted for apples. I speak very little Spanish, so asking the clerks in the store about each fruit, its taste, how to eat or prepare it wasn’t really an option. Read More...
Staying simple
 A few months ago, I wrote a post about my personal development as a counter-piece of anecdotal evidence to those examples suggesting poorly supported complexity and expense to achieve a body transformation.
A few months ago, I wrote a post about my personal development as a counter-piece of anecdotal evidence to those examples suggesting poorly supported complexity and expense to achieve a body transformation.
Anecdotal evidence is considered the lowest quality of evidence upon which to base decisions. It is highly susceptible to sampling bias (most people who don’t get the outcome they want don’t tend to tell their story), selection bias (I get to pick the best pictures), recall bias (most people aren’t that great at keeping research-level records of all the factors contributing to their story), as well as out-and-out dishonesty; but when it comes to individuals making decisions, it also seems to be one of the most powerful and potentially driving pieces of evidence. It is something that I think I would like to study in the future (collaborators welcome!), but as an idle musing, I think anecdotes are so powerful because they are generally quite personal, and very accessible. Anyone can read a story. There aren’t really any statistics that require courses or books to decipher. And when it comes to basing a decision on an anecdote, there aren’t any right or wrong answers. You can decide to use an anecdote because you think it fits your circumstance or not; either way, you’re right because there are so many ways in which an anecdote can fit, or not fit your situation. Read More...
Control is where you find it
 When I was my first year of residency, I did my 8-week neurosurgery rotation. I have all the respect in the world for neurosurgeons (I mean, apart from the blatant overuse of the “This isn’t brain surgery…” joke), but neurosurgery is not for me. Everyone thinks ICU is the most intense, but it’s not–at least, not for me. I remember being so tired and so busy and dealing with so many sick patients that about 3 weeks in, I started having what I’ve described to my friends as, “elevator escape fantasies” where I fantasized getting onto one of the hospital elevators and getting trapped inside, unable to answer my pager and just being able to curl into a little ball on the floor to get some sleep. That’s right. Some people’s terror-filled nightmare was my escape fantasy. I would take the elevator all of the time (except for real emergencies) on the off chance that I would get stuck. It never happened. And eventually, the rotation came to an end, and I lived to tell the tale.
When I was my first year of residency, I did my 8-week neurosurgery rotation. I have all the respect in the world for neurosurgeons (I mean, apart from the blatant overuse of the “This isn’t brain surgery…” joke), but neurosurgery is not for me. Everyone thinks ICU is the most intense, but it’s not–at least, not for me. I remember being so tired and so busy and dealing with so many sick patients that about 3 weeks in, I started having what I’ve described to my friends as, “elevator escape fantasies” where I fantasized getting onto one of the hospital elevators and getting trapped inside, unable to answer my pager and just being able to curl into a little ball on the floor to get some sleep. That’s right. Some people’s terror-filled nightmare was my escape fantasy. I would take the elevator all of the time (except for real emergencies) on the off chance that I would get stuck. It never happened. And eventually, the rotation came to an end, and I lived to tell the tale.
When I think back on those really tough weeks, there was a lot that I couldn’t control. I can tell you what I couldn’t control: I couldn’t control when to work out. I couldn’t control when to study. I couldn’t control when to go home, or when to wake up (4:30am, if you must know). I couldn’t control when to eat. On call, I wasn’t even in control of my sleep. To a certain degree, nothing has really changed since those neurosurgery days. I have a little more control, but just last week, we were up until 4:30am re-attaching a thumb. But even in that chaos, there were things that I could control: I could control WHAT I ate. I could decide to work out on days that I wasn’t on call (on the days I was DOG tired, I could decide to just walk INTO the gym and let the workout fall as it would). And I could control my decision to take the stairs or the elevator (The elevator, always the elevator, because you really can’t get stuck in a stairwell–AND people are more likely to notice an elevator not working and therefore, find you, whereas getting stuck in a stairwell most likely means something bad has happened to you…See how thoroughly my fantasies are thought out?) Read More...
Restriction: It’s not just for calories
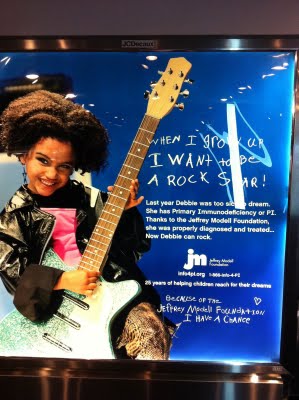 I’m sitting in the Newark airport and having a sandwich at the Earl of Sandwich (it’s the only place I can sit down here, it seems). There was a sign as I came up the ramp for “PI” stating that “He’s a child isn’t a diagnosis”, implying that your child’s cold could be a sign of “PI”. As I’m sitting here eating this club sandwich, there’s another sign outside the restaurant also for “PI” or “Primary Immunodeficiency”.
I’m sitting in the Newark airport and having a sandwich at the Earl of Sandwich (it’s the only place I can sit down here, it seems). There was a sign as I came up the ramp for “PI” stating that “He’s a child isn’t a diagnosis”, implying that your child’s cold could be a sign of “PI”. As I’m sitting here eating this club sandwich, there’s another sign outside the restaurant also for “PI” or “Primary Immunodeficiency”.
Primary immunodeficiency is a condition that affects (at best estimate) about 1 in 100 000 births. There are at least 5000 people that see that sign every day. Of those 5000 people, a much lower number of them will have children and even lower still, the number of those individuals who have a child less than 1 year old. In 20 days (almost a month), that sign would be applicable to a single individual if they were all infants under the age of 1. How many days would it take to pick up one case of PI? Probably more than 6 months to a year. Important? Yes. Because PI or SCID (Severe combined immunodeficiency) can result in DEATH before the age of one year if untreated. Read More...

Flukes–more than fish.
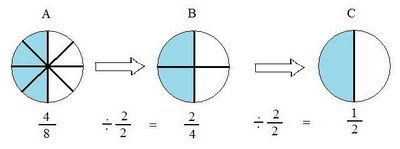
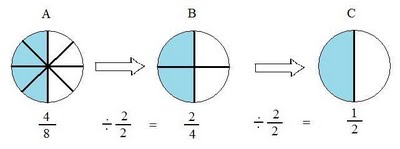
 In January this year, I was in Cancun at a conference (I know, life is harsh). We were traveling from the hotel to the conference and my friend David gave me half a peso back in change because I had lent him too much for bus fare. I said flippantly that he could keep the “half-cent”. He pointed out to me that half a peso was more than half a cent, and was, in fact, 5 cents, or a nickel. I said it was barely more, and he rebutted that it was TEN times more. It was then that I realized this was a very good illustrative example of how a statistically meaningful difference still doesn’t translate into buying a pack of gum.
In January this year, I was in Cancun at a conference (I know, life is harsh). We were traveling from the hotel to the conference and my friend David gave me half a peso back in change because I had lent him too much for bus fare. I said flippantly that he could keep the “half-cent”. He pointed out to me that half a peso was more than half a cent, and was, in fact, 5 cents, or a nickel. I said it was barely more, and he rebutted that it was TEN times more. It was then that I realized this was a very good illustrative example of how a statistically meaningful difference still doesn’t translate into buying a pack of gum.
Most of the studies I review for this site fall into two categories: Read More...
Anecdotal Evidence-Based Fitness

And at some point in every fitness-writer/blogger’s lifespan, there has to be come form of accountability for what he or she writes. A proponent of supplement X should probably be using supplement X and not just writing in favour of it to get paid if they really think it works. A writer who believes in workout A enough to rave about it should probably be able to show that it works at least for themselves. It’s of little value to say, “X totally works and everyone should be using X, but I don’t.” Read More...